
A Blog Article about the Challenge of ECOLAH
By Paul Beenen and Marije Bosch
This blog is about the challenge of ECOLAH, an Erasmus+ funded project in higher education which stands for Embracing Complexity Oriented Learning Approaches in Health. ECOLAH’s ambitious goal is to co-drive the transformation to a healthier society by acknowledging the role of higher education in it. Currently, we feel higher education systems do not sufficiently prepare students to contribute to the many major societal challenges we face. We pose that if higher education takes their societal role seriously, itself will need to undergo transformative changes as well and embrace systems-thinking and complexity-oriented learning approaches.
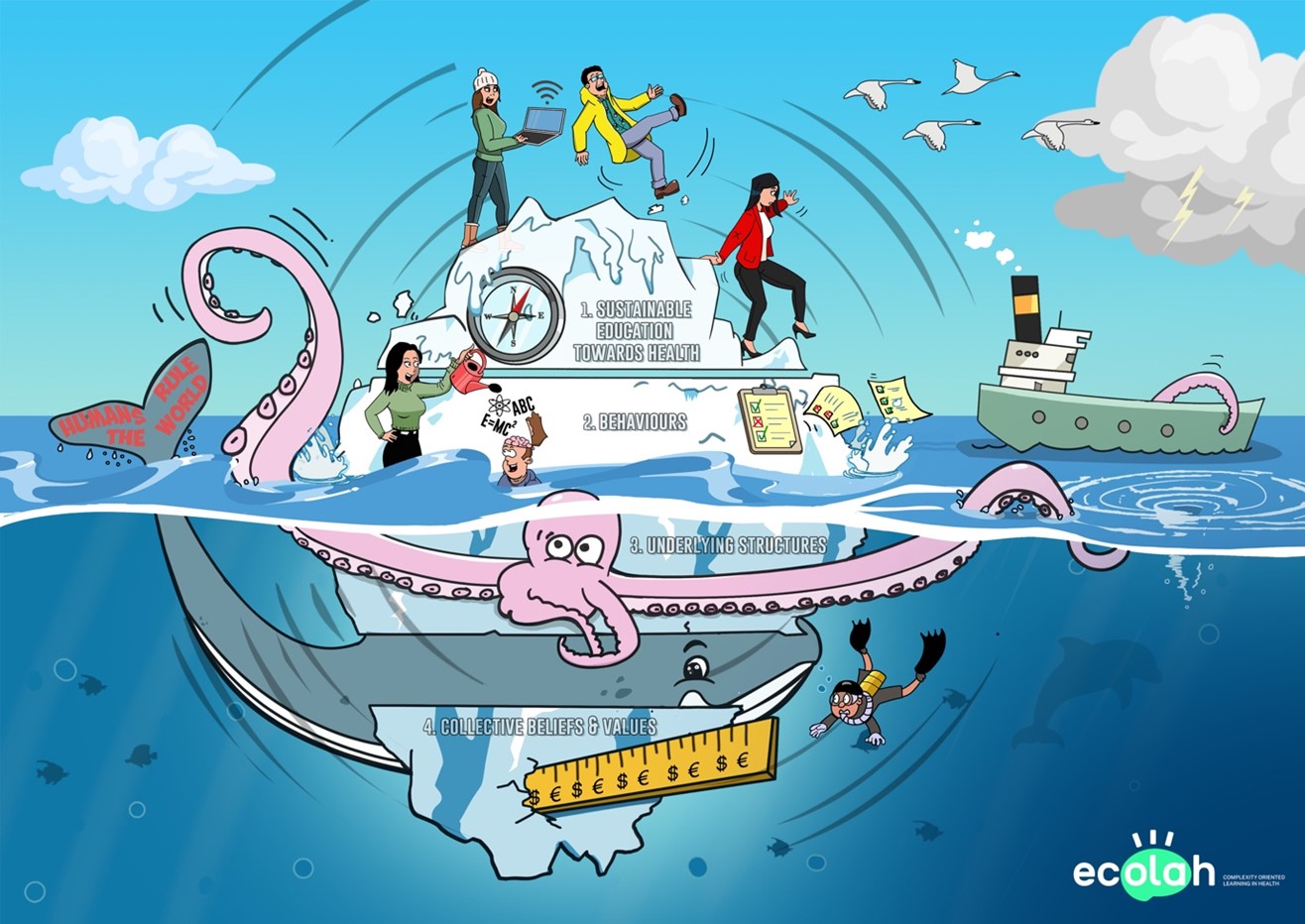
In writing about the challenge of ECOLAH, we use the Iceberg Model to structure our story (Inayatulla, 2005). It is a systems-thinking tool that can be used to understand the underlying causes (typically hidden below the surface) of an event or situation. Our iceberg contains four layers (see illustration). The starting point for our story is the tip of the iceberg (layer 1). It is clearly visible above the water and represents the surfacing challenge: sustainability education towards health. Here, we talk about what we consider sustainability education, why we think sustainability education is needed and why we place complexity and systems-thinking at the heart of it. Why we consider this a challenge indeed becomes apparent if we dive ever deeper beneath the surface to shine a light on the underlying behavioural patterns (layer 2), structures (layer 3), and beliefs and value systems (layer 4). These are often less apparent and more implicit (hence below sea level). Directions for meaningful and transformative changes will need to address not just what’s apparent, but also the incentives and motivations that caused the challenge in the first place. Only by diving below the surface one gets to see the bigger picture. We also point to some directions for solutions. We finish this blog with a brief preview of the direction ECOLAH is taking.
An iceberg does not exist in a vacuum. The context in which it floats represents the “sea of possibilities”; the myriad of future directions and pathways that are or become possible. The sea serves as a metaphor for the journey we experience on our way to complexity-oriented education and the systems we operate in. The sea is never still. It always moves. Its currents are influenced by coastal and sea floor features, winds, and tides. In turn, they influence climate zones and weather patterns around the world. The vastness of the sea contains surprises such as whirlpools which may throw the iceberg out of its current stream into another future path.
Layer 1: the challenge of sustainability education in health
The tip of the iceberg represents the challenge of designing educational practices that embrace systems-thinking and complexity. Our societies are currently facing multiple interconnected crises such as loss of biodiversity, climate change, and ever-increasing gaps in income and health equality. ‘Solving’ these crises is far from easy. They require ‘sustainability transitions’: large scale disruptive societal changes (Loorbach, 2017). Sustainability transitions emerge over a long period of time (decades rather than years). They will fundamentally change what we do and think and how we organise our societies (the underlying layers of the iceberg).
Transformations are inherently systemic and complex. Therefore, to navigate transitions it is important to understand how complex systems work. A ‘system’ is created when actors form interdependent relationships. The action of one actor then has implications for the other connected actors. The system becomes ‘complex’ because the interdependencies that define the system also cause it to be highly dynamic (Cohn, 2013). In complex systems, a small change may create large and sometimes unanticipated effects (the law of unintended consequences). It is impossible to ‘extract complexity out of a system’ as it is a feature of the system itself. It is also impossible to dissect a complex system and reduce it to neat parts without losing its meaning. For example, a bike can be dismantled, understood as separate parts, and put back together again. An elephant cannot. In a complex system, the whole is larger than the sum of its parts. Systems thinking is a way of making sense of the complexity of the world by looking at its functioning in wholeness and relationships rather than by splitting it down into its parts.
In health, transformative change is needed where health is no longer seen as something that solely belongs to healthcare systems but is seen as an intrinsic value in everyday life that needs caring for (the transition from ‘healthcare’ to ‘the care for health’ (Beenen, 2022)). This ‘caring ethics’ applies to people but extends to the systems humans are interwoven with – the planet and all its inhabitants. This requires a paradigm shift in how we see health and what we value in life. What the future will exactly look like is unknown and unknowable. The ethical consideration to actively work towards societal change and a better, more just and sustainable future (rather than accepting and teaching the status-quo) is a normative decision. It gets us on a path of wayfinding. This is a long-term process in an ever-changing context (symbolised by the fact that the iceberg is turning). The compass in the illustration symbolises that this path is not a paved road. Rather it is a direction for the collective learning process in which we continuously study what is working to get us to the desired future and what isn’t. Logbook entries will be placed along the way to share lessons learned with others. These learnings are place-based. What works in one context may not work at all in another, depending on the local circumstances. Here, context matters.
We feel that, in general, our higher educational systems are underperforming when it comes to preparing their students to navigate the complexity of the world and creating agency for meaningful change. As Stephen Sterling, in his essay “Educating for the future we want” (2021) states: “If education is to be an agent of change, it has itself to be the subject of change. Our educational systems are implicated in the multiple crises before us, and without meaningful rethinking, they will remain maladaptive agents of business as usual, leading us into a dystopian future nobody wants.” Students will need to learn how to design long-term wayfinding processes and monitor those along the way. Learning takes place in the collective, but also individually. As part of the process unexpected things will happen. They will need to learn that not everything can be pre-defined and planned for. That in complex situations, the linear cause-and effect-relations don’t hold. That it may not be possible to ‘solve’ the challenge in the first place, as new issues will pop up that require a constant process of ‘relating to’ – rather than ‘fixing’. They must learn how to develop knowledge and lessons learned in a particular context and ensure all relevant stakeholders (including the planet and non-human inhabitants) have a voice in the process. They will need to become comfortable with ‘not knowing’, with studying relations and patterns. In short, we need ‘sustainability education’; education focused on societal change, using complexity-oriented learning approaches (Sterling, 2021). But as Greenhalgh (2018) puts it: “It is fashionable to talk of complex interventions, complex systems, complex patients, wicked problems, and the like. However, with few exceptions, we embrace the theme of complexity in name only and fail to engage with its underlying logic”. ECOLAH aims to contribute towards this challenge by co-creating tools and approaches to learning that are congruent with our assumptions regarding how the world works and what constitutes knowledge. These approaches can then complement the more conventional educational practices. To illustrate our assumptions regarding the underlying causes of the challenge, we now dive below the surface.
Layer 2: Behaviours
The second layer is the layer of (mostly observable, but partly hidden) behaviours; the dominant approaches in the current higher educational systems. Here, we highlight some observations in relation to our current educational practices which hamper a complexity-oriented approach.
First, ‘teaching’ students is mainly practiced as a transfer of ‘a package of knowledge’ from an expert (the teacher) to a novice (the student). In our illustration this is visualised by a teacher pouring knowledge into a students’ brain. Freire, in his book “Pedagogy of the oppressed’ (1970) calls this ‘banking’. Banking assumes that all knowledge can be objective (knowledge about something, developed ‘from the outside’) (Beenen, 2019). When learning about complex challenges – the learning needs to be more active, and situation and place-specific (knowledge being construed and having meaning in the context, in a sense-making process with all relevant stakeholders).
Second, students learn to think ‘linear’. For example, medical students are taught to arrive at a diagnosis and then select the intervention that is most likely to help. This implies a predictable linear cause and effect relation between ‘problem’ and ‘solution’. Related to this, knowledge is bound to ‘subjects’. This reflects how we organise the world; academics study narrowly defined scientific areas and curricula have become so specialised and fragmented that more systemic societal crises are being easily overlooked. Medical professions for example have become more and more specialised. So, a patients’ health is reduced to one perspective. Often, the clinical reality is much more complex. Patients have co-morbidities. How to treat patients with seven diagnoses? Patients live in socio-cultural environments that influence their health. How to factor that in?
Third, in general, students know exactly what they should expect from their courses and what they need to know at the end of it (visualised in our illustration by the checklists). This is in stark contrast with teaching the value in ‘not knowing and ‘anticipating emergence’ and collectively deciding in a wayfinding process which knowledge is needed. Learning outcomes are generally pre-defined and captured in detailed rubrics. This does not match the reality of active learning, which tends to be ‘messy’: partly invisible, unfocused and unsettling – and taking place ‘in the dark’ (Dall’Alba, 2019).
Finally, the knowledge being tested is knowledge that can be measured – which may not correspond to what is important to measure. For example, creativity is considered an important competence in learning in complexity. But how do we measure this? Would it mean anything to score 5.4 on the ‘scale of creativity’?
Layer 3: Underlying structures
The layer just below the surface of the sea talks about the underlying structures (such as power structures, infrastructure, policies, and rules) underpinning the behaviours. Once ideas have been institutionalised, things work a certain way (path dependency). Transformative change is so hard because the current ‘regime’ is exerting its power to keep things the way they are, in predictable and thus controllable, ever deepening, grooves. The Leviathan in our illustration (in the shape of a formidable octopus to refer to our entwinement in the web of life) is a metaphor for an alternative movement, which supports and facilitates the emerging alternative structures and practices (by using some of its tentacles to swing the iceberg), but also actively works on dismantling existing unsustainable regimes (Loorbach, 2014). Here, we highlight some characteristics of the current regime hampering change.
First, the main orientation of the services which higher education institutes deliver is ‘supply-based’ in the form of standardised courses taught behind academic walls and research focused on academic output rather than societal impact. Although the higher education sector increasingly acknowledges its role in serving local communities, mostly, the infrastructure to collaborate with societal stakeholders, as part of an ecosystem, is still rather rudimentary. In sustainability education, primacy is given to informal learning in the real world. Formal education will need to adapt to that, by integrating formal education into these more informal learning processes. Governance and financial structures are often impeding this; higher education developed as independent institutions with their own domain specific ‘external’ accreditation process. The laws governing higher education institutes are often ensuring ‘quality control’ and ‘standardisation’, thereby limiting the conditions needed for true lifelong learning: the flexibility to develop education based on societal demands and integrate this with research and innovation within real world challenges.
Second, and related to the previous point, for transitions and complex challenges many different perspectives and transdisciplinary solutions are needed. So, ideally students of all different backgrounds learn together. Universities, however, are organised in Faculties. For teachers, it would require more time and coordination to develop these forms of learning, while the incentives are on efficiency and cost containment.
Third, current staff qualification and faculty development programs do not include complexity-oriented learning approaches. We feel this is a major hurdle. In the banking model, teachers are the experts. They decide which literature is important, and so, who are the knowledge holders. In collective wayfinding, knowledge is situational, short-lived and negotiated between many stakeholders in a democratic sense-making process. Here, a critical pedagogy is needed, in which a plurality of knowledge systems is embraced and used to arrive at answers, questions and solutions that benefit all. Teachers then need to become learners in the collective as well. This may be confronting and uncomfortable for some as it would shift the power balances and existing systemic inequities. It would also require teachers to grow into a different role (mentoring rather than teaching and cultivating a safe learning climate where evidence informed experimentation is cherished).
Layer 4: Collective beliefs, culture and values
Ultimately, it is what we value as a society that determines how we organise ourselves. The final layer is the one with our collective belief systems, culture and value systems. So, here we highlight some cultural traits that relate to how we see the world.
First, in the Western world, the age of Enlightment was marked – amongst others – by an emphasis on the classic scientific method and reductionism. This had led to a focus on reductionist Newtonian-style thinking (linear cause-effect relations), in which complexity is reduced and controlled for. Research is being seen as conducted by a ‘subject’ ‘objectively’ studying ‘an object’, without taking the context into account. This naïve, positivist interpretation of what constitutes knowledge is symbolised by the ruler in our illustration. For sustainability education, a shift is needed to a systemic view of the world, with continuous attention to the relations between actors and the anticipation of emergence. The unpredictability of innovation means that data collected using historically important categories and measurement instruments will not suffice as it will miss things of importance. In an industrial age, with highly standardised production processes, it was possible to simply ‘apply knowledge’ (hence the banking metaphor). However, in a diversified landscape, practical application requires the active and social capacity to create knowledge and make sense of it in the context in a dialogical and democratic process. This requires a shift to a more pragmatic, evaluative, critical epistemology. Learning, then, is about the ability to create and invent practically relevant knowledge. So, we will need learning methods and strategies to support this.
Second, and related to the first point, learning is generally considered a ‘consumption article’, (strongly induced by neoliberalist assumptions). The education ‘product’ is sold to an individual learner (the potential buyer: the aspirant -often young- student). The fact that students know what they need to learn at the onset of their educational programs has led to expectations of teachers transferring all the relevant information and students -rather passively- simply ‘consuming’ their input. Education is then avoiding the ‘pain of education’, especially when confronted with learning in complexity, as this will negatively influence their consumers satisfaction. This is not in sync with the societal demands.
Third, an individual and human-centred frame (visualised by the graffitied whale trapped in our iceberg) has contributed to a narrow view on individuals and parts, projects and sectors. For truly sustainable solutions, we will need a frame focused on wholes and learning of the system as an interwoven web of life (Guzman, 2021).
ECOLAH’s OWN WAYFINDING PROCESS
The sea water in which our iceberg floats is steadily warming up. The challenges in health and higher education are becoming increasingly urgent. However, the behaviour of academia is only marginally warming up to be complexity-orientated. Progress here seems utterly slow. Teachers/academics “are at least partly complicit in shaping and even perpetuating some of the complex and challenging crises facing the university and the world, and consequently, humanity’s hope of building a more sustainable future” (Naidoo, 2015). UNESCO, in 2021, stated that we face the challenge of “realizing the transformational potential of education as a route for sustainable collective futures. To do this, we need a new social contract for education that can repair injustices while transforming the future. This new social contract must be grounded in human rights and based on principles of non-discrimination, social justice, respect for life, human dignity and cultural diversity. It must encompass an ethic of care, reciprocity, and solidarity. It must strengthen education as a public endeavour and a common good.
To work towards a situation in which conventional education is being complemented by sustainability education, all layers of the iceberg should be considered. ECOLAH focuses on the learning in complexity and serves as an example of an alternative frame for the system to evolve into. We will co-create courses and tools clustered around themes we consider central to learning in complexity. In doing so, we should practice what we preach and use transformative research methods to evaluate our process, in which the active learning in the context with all stakeholders is taking centre stage. Some of the learning questions that arise include:
* How can we develop local learning spaces based on informal learning with support from formal learning processes and research and innovation projects?
* How can we develop faculty (curricula, teacher competences, governance) towards learning in complexity?
* How can we develop further towards an evaluative culture rather than a testing culture?
* How can we increase the readiness and capacity to grasp the urgency of learning in complexity and the necessary (interwoven) changes on all levels of the iceberg and its environment?
We aim to arrive at narratives of change, captured as local case studies, as stories are a good way to capture locally relevant lessons learned. As Greenhalgh (2018) puts it: “Decisions must be made on the basis of incomplete or contested data. People use their creativity and generate adaptive solutions that make sense locally. The articulations, workarounds and muddling-through that keep the show on the road are not footnotes in the story, but its central plot. They should be carefully studied and represented in all their richness.” [see list of references in download document]
© 25-10-2023 by Paul Beenen, Marije Bosch is licensed under CC BY-NC 4.0


