A TRAVEL REPORT FROM A HIGHER EDUCATION COURSE EXPLORING LEARNING IN COMPLEXITY.
A reflection from Maaike Huizing and Marleen van Dijk
Management in Healthcare is a BSc programme in the Hanze University in Groningen, the Netherlands. Part of the course is a learning unit called: It’s a wicked world of 5 European Credits. The aim of the course is to train the capability of students to understand, anticipate and act in congruence on the complexity of health care and the necessity to work towards a transition of health in the role of a manager.
This course is a context in which learning in complexity plays a major part and within the ECOLAH project it will be the environment where the concepts and learning units will be piloted. The course ran from September till November 2022, and we have been using the inspiration and concepts from learning in complexity for experiments in the class room.
We will be part of the Training, Teaching and Learning Activities (TTLA) and viewed this new learning unit “It’s a wicked world” as a case to experiment with the concepts discussed in the kick-off meeting of ECOLAH.
For this we formulated the following learning questions:
can we design a learning space in the course Management in care what offers learning in complexity.
How do we facilitate this learning?
This resulted in a travel report based on lessons learned we formulated as a kind of guided principles. We hope to discuss the lessons learned and some learning questions when we participate in ECOLAH’s capacity building (TTLA) in January 2023 in Bergen.
A LEARNING PATH IN COMPLEXITY AND FUTURES LITERACY.
By Paul Beenen and Loes Damhof
This blog is the summary of two key notes during the final conference of the HIPPA project in digital innovations at the Metropolia University in Helsinki, October 2022: We felt both key notes were complementary and an example of the necessity to fundamentally rethink our world view, our perception of knowledge and agency facing the great challenges around health and social care today. We will argue for this rethinking and for the capability of futures literacy as an essential asset in this process of learning.
As such, this blog also illustrates the underpinning of our project ECOLAH, that stands for Embracing a Complexity Orientated Learning Approach in Health. A European project that explores the consequences for learning when we take the underlying logics of complexity seriously. For more information, follow us on this website.
The care for health is crumbling fast
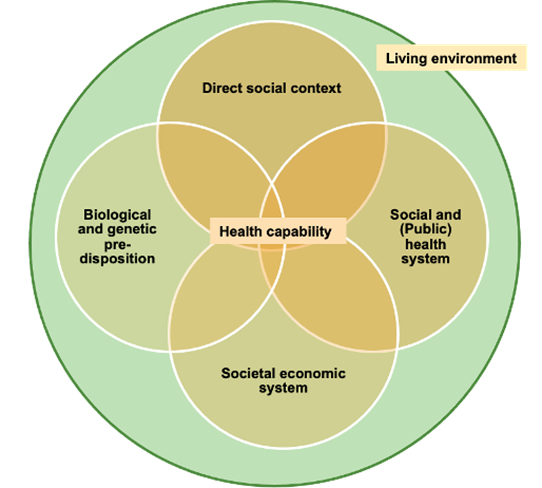
Health and social care are in general based on a diagnose-intervention thinking. Once a problem arises, we determine the problem (diagnose) and then find a remedy (intervention). This has shown to be an extremely successful mode of thinking resulting in increased longevity and the ability to “manage” a diversity of health problems. Although successful, the last decades have proven this is not enough. Healthy life years turn out to be the result of a web of factors constantly interacting with each other (figure 1; based upon Prah Ruger, 2010; Bellancasa, 2017).
All these factors such as the influence of socioeconomic status, a societal tendency towards unhealthy stress induced lifestyles and the continuous neglect of the health of our planet, impact the health of people massively. Most individual health problems are chronic and are increasingly impacting our lives, often impairing us along the way. We are basically waiting till we are sick enough to be diagnosed before the system allows us to do something about it. We define urgency in health only when the damage is done:when a health problem occurs, it is often too late for the majority of societal health issues. While dealing with one health issue, people are often deconditioned and become highly vulnerable for other chronic lifestyle induced problems. Being lonely for example, fosters an inactive lifestyle which in return can increase health risks.
To put it bluntly; health and social care systems are designed to take care of health problems but do not invoke the capacity to be and stay healthy. The way modern societies have developed in the last century and the associated health problems have received little attention. We often start to hear the call for urgency when a problem has developed over decades into a storm we can’t ignore any longer. These systems are financially unsustainable and unable to answer the demands of society. Moreover, challenges like the increasing demand of health workers under a high demographic pressure, the pandemic of Non-Communicable Diseases and a deteriorating planetary health have been known for decades, without any actionable result to speak of.
It is therefore not surprising that health systems are under tremendous pressure of being unable to deliver the necessary services while dealing with increasing costs. Optimising the current health systems will not suffice and won’t reach SDG 3;Ensure healthy lives and promote well-being for all at all ages. Policies to incrementally change this undesired and unsustainable situation doesn’t expedite these reforms (Christensen et al, 2017). An alternative is the fundamental change from solely problem oriented ‘health care’ towards the care for health.
Taking complexity of health seriously
Taking the care of health seriously necessitates the acknowledgement of the interweaving and dynamics of all factors as a complex system. Questions of circumstances, events, timing, history, personal and cultural preferences matter enormously in addressing the question ‘what needs to be done? (Tsoukis, 2017). However, as Greenhalgh points out; “It is fashionable to talk of complex interventions, complex systems, complex patients, wicked problems, and the like. However, with few exceptions, we embrace the theme of complexity in name only and fail to engage with its underlying logic” (Greenhalgh, 2018).
To understand better why we have so much difficulty navigating complex systems, we need to distinguish between complicated complex and complex issues. A problem that is complicated means outcomes and effects are predictable and effective actions can be planned and translated through guidelines into actions (e.g. a cookbook). The great attraction and success of this view is that we can predefine the outcomes, and thus control and audit processes and results. An example of a complicated issue is an open heart operation, a tough challenge but with the right manual, knowledge, and material you can exactly get what was envisioned (and thankfully so). Our diagnose -intervention based health care systems are fully built on this complicated world view. In complex phenomena, like raising a child, the outcomes can often not fully be (pre) defined from the beginning and the steps to follow are always situative, negotiated and follow non-linear patterns. Simply said ‘context matters’. This complexity could be defined as: “A dynamic and constantly emerging set of processes and objects that not only interact with each other, but come to be defined by those interactions” (Cohn, 2013).
Don’t make from a complex issue a complicated one
The practical consequence of dealing with complex issues is that we, (managers and controllers included), need to accept that we do not know everything, which leaves us with the need to constantly anticipate these ‘emerging sets of processes and objects’ with a certain amount of uncertainty. What is left is a humble learning process navigating complexity. This thinking feels counter-intuitive to a reductionist diagnose-intervention mindset: the first reflex is often to reduce this complexity to a complicated problem by focusing on one or more ‘determinants’. This explains why health professionals tend to reduce a whole, complex human being, into a patient as if it were a single identity (and then follow the guideline). This is why the global health community responded to the COVID pandemic with a sole focus on finding a vaccine, while largely neglecting the rest of the societal system.
Learning in complexity
Accepting the underlying logic of complexity offers an opportunity to think beyond linear causal problem solving. Complex systems have the property to self-organise and adapt to new situations. A hopeful example was the caring resilience of local communities during COVID and lockdown. Care emerged from local communities, neighbours were shopping for each other and alternative ways of social contact and physical activities popped up. Tapping into this adaptability is an explorative, creative ‘trial and error’ way of learning. It’s less controlled, sometimes downright messy, and highly dependent on the local situation. Do we still have the space and degrees of freedom to engage in such a journey, to experiment, to allow for mistakes? How do we integrate systems thinking in our approach towards the care of health, from patients to the whole health system?
A major support in (re-)learning to think with this complexity is to accept that our knowledge is not all static (objective) and can not be planned and controlled. In complexity, knowledge is often short lived and depending on the dynamics in the system. This is uncomfortable as it demands a constant monitoring and evaluative attitude towards what we consider knowledge of the situation. Learning in complexity is then wayfaring; negotiating or improvising a passage as we go along. Knowledge is then grown along the myriad paths we take as we make our ways through the world in the course of everyday activities, rather than assembled from information obtained from numerous fixed locations (Ingold, 2010). This is uncomfortable as it demands a constant monitoring and evaluative attitude towards our knowledge of the situation. It is even more uncomfortable because we can’t put our objective truths upon people and systems. Not without accommodating towards the woven web of what we call ‘context’ with all it’s historicity, dependencies and dynamics. Yet, this more humble position offers also a way to understand and respect much better the qualities of our interconnected world and to cherish its agency. The hardest nut to crack is to say farewell to our illusion we can plan and control, if not colonise, our future. For this it is important to invest in futures literacy.
Futures literacy
Futures Literacy is the capability to imagine multiple futures to see the present anew. Fundamental to this capability is acknowledging that the future does not exist. It is the undefined later-than-now (Miller, 2018)and the only way the future takes shape in the present, is through imagination. The future is fiction, and yet it has a profound impact on what we do, how we think and act in the present. It is therefore time to think about how we think about the future.
Anticipatory systems
Although the future does not exist, we use her every day: to plan our week ahead, to schedule appointments, to dream about that trip or to worry about our health or age. These are common ways to use the future, or in other words to anticipate: we might plan for something we see as preferable, or we prepare for something we deem necessary or plausible. We call these ways of using futures anticipatory systems (Miller, 2018). What they have in common is a certain idea of what the future might hold; a scenario, a dot on the horizon, a strategy or a dream. These ideas, scenarios or stories we tell ourselves are based on a variety of factors: upbringing, culture, films, books or education. Think of our assumptions of what a healthy person looks like, or what healthcare should entail in a modern society. These narratives are rooted in systems, worldviews, myths or metaphors, and can often be static or deterministic (Inayatullah, 2015). Many (digital) innovations in healthcare for example, albeit useful and life-changing, do not change the system or worldview that lies underneath. A new technical tool can solve problems in the short run, but does not change the way we see health in society. To put it bluntly: everybody wants change, but nobody wants TO change.
Challenging dominant narratives
To fundamentally change how we see care for health, or what it means to be healthy or to be able, we need to start with our shared narrative of the future. What is it that we fundamentally believe in? These visions of the future shape our decision making in the present: they offer guidance, or can stimulate our sense of agency. They can, however, be extremely limiting in our capacity to innovate, to be creative and open to uncertainty and novelty in the present. Without understanding what assumptions or static narratives we base our futures on, we fail to detect our blind spots, or to see different ways of doing. It’s when ‘how we respond to a problem, might become part of the problem” (Akomolafe, 2016). Think about the topic of the HIPPA conference Digital innovations for the future of housing seniors: based on what assumptions do we intend to foster these innovations? That the word ‘senior’ has the same meaning in the future as it has now? That we still live in houses ? That technology continues to develop the way it has? Controllable by mankind? To identify these anticipatory assumptions we need to engage in a different anticipatory system besides planning and preparation. We can use the future for exploration by thinking about the unthinkable, imagine the unimaginable, by exploring alternative scenarios that may seem whimsical or farfetched, but can help us stretch our imagination beyond the obvious and help us identify the gaps in our thinking. Reflective practices are key here, as is the collective intelligence when engaging in these sort of exercises. Listening to the different futures of others and their interpretations can push our imaginary boundaries even more. The future does not exist, but thinking about her does and by widening the pathways in front of us, we are able to see more in the present. It can help us to overcome the poverty of imagination.
Walking in two legs
The practice of exploring alternative futures to see the present differently is called anticipation for emergence (Miller, 2018). When able to navigate between the three anticipatory systems (planning, preparation and exploration) in different contexts and for different purposes while identifying anticipatory assumptions, one can be called futures literate. Miller calls this ‘walking on two legs’, as we need both, anticipation for the future and for emergence. This capability, as any capability, takes time to develop and while practising, one should resist the modern call for urgency or for acting on an impulse. Understanding the differences in these anticipatory systems can force us to challenge the status quo of the current health care and social systems, and can make space for a different kind of (shared) decision making. Less controlled, less focus on complicated problems but more personalised and appropriate for any given situation; an approach that demands learning in complexity.
Futures Literacy accepts the premise that the future cannot be foreseen, and that knowledge creation is dynamic and fluid. It allows for complexity to be appreciated, not to be solved, and for uncertainty to be embraced, not to be eliminated. It enhances our perception of the present: we sense more, but novelty also makes more sense. Lastly, it changes our sense of agency (Kazemier et al, 2021), as we make better informed decisions and become comfortable with different ways of being, thinking and doing.
Wrap up
We state in this article that we should take the care of health more seriously as a grand societal challenge. For this we need a worldview that embraces more the underlying logic of its complexity (ontology) and be consistent in how we get and value knowledge of this world (epistemology). Learning in complexity offers a nascent guideline on how to do. Its goal is to install a humble yet performative attitude of ‘wayfairing’, developing capabilities and supportive learning methods. Futures Literacy, named by UNESCO as the essential capability of the 21st century, can help us change the narrative from health care to care for health.
CHALLENGING OUR REFLEX TO REDUCE COMPLEX ISSUES INTO CONTROLLABLE COMPLICATED ONES.
News article from Hanze UAP about the E+ funded project Suswell
SUSWELL stands for sustainable wellbeing. It is a European project in which the European Union helps Russia and Kosovo to better organize their health care welfare. Paul Beenen, Margarita van Dijk and Jos van Kempen talk about the value of European collaboration on complex themes in healthcare and welfare.
THE PROJECT LEADER
Paul Beenen is a professor-researcher at the Institute for Sports Studies and the Academy of Health Studies and project leader at SUSWELL. “Keeping a dialogue about European values and looking at what we can do for each other. Germany Portugal, Finland, Belgium and the Netherlands are connected in SUSWELL. We are doing three projects in Russia. In Saint Petersburg, Perm and in Belgorod, which is 15 kilometres from the Ukrainian border. And two in Kosovo, in the capital Pristina and Gjakova. Russia is of course difficult right now. Formally, we are not allowed to work with institutions that belong to the state, and almost all of them are. We also have NGO partners and partners from a private institution, and you are still allowed to work with individuals. Half of our partners have fled because they have different ideas than Putin. Communication is also becoming increasingly difficult. If there hadn’t been a war, I would have been in Perm this week.”
Community of Practice
SUSWELL is building a community of practice around an urgent health theme, in which citizens, knowledge institutions, local government and companies participate. Together they look at an issue. Paul: “We initiate social and local changes. We tackle what is locally urgent. In Gjakova it is about women who experienced sexual violence during the war. In Pristina about children with autism, who disappear in the periphery and who are given insufficient opportunities to participate in society. It is interesting that we in the Netherlands can also learn a lot from this. We often act as if we know how to do it, but even in the Netherlands children with autism sometimes fall through the cracks. Some things they just do better abroad. Because healthcare is sometimes less well organized, informal care is often better organized.
Looking critically at your own context
“One cannot solve complex issues in healthcare and welfare on their own. By looking at a different context, you also look more critically at your own context. Due to scarcity, because there are few facilities, you will work together more locally. In Groningen, more and more facilities are disappearing from the province, while more and more elderly people live there. We have to get people used to the fact that not all facilities are around the corner anymore. For example, we are also poorly geared to remote monitoring, they are much better at this in Russia and Finland, because they have to deal with greater distances.
THE PROFESSOR
The Dutch Margarita van Dijk and her family have been living in Kosovo for ten years. She teaches Physiotherapy and is responsible for the Occupation Therapy programme within the Kolegji Heimerer, the Faculty of Health of a private University in Pristina. Kolegji Heimerer has a therapeutic centre where children with autism are treated. “We are working on autism at all kinds of levels”, says Margarita via Teams. “We want to take a good look at the role of these children in society and what we can add to it. We investigate what children need outside of therapy to be able to participate successfully in society. We do this by bringing stakeholders together. People who are responsible for their part in the picture of autism, such as the government, NGOs, education, therapists and parents. Children with disabilities are generally hardly included in society here. Parents sometimes don’t even want to hear that their child has something. It’s a bit of a shame. For parents who do see this, and experience it as a burden, there is often no help at all. There is no luxury in Kosovo to offer the child what it needs.”
Hope
“It gives parents in Pristina hope that so many different people are thinking about autism. That teachers know that the government thinks along, and parents that therapists think along. We have mapped out the bottlenecks and the opportunities together with the stakeholders. The lack of extra help at schools is a problem for both teachers and parents.’
Practice-oriented education
Margarita: ‘In the field of education we are working on new themes such as futures literacy. How do we look to the future and how are we going to approach it differently now? To do this, we receive more in-depth knowledge from our mentors, so that we make education more practice-oriented. We hope that we can also apply the concept of the community of practice to other target groups. Kosovo has a lot to offer, but there is still a lot to gain in terms of cooperation. People here really want to think and act towards Europe, so we are always very interested when there are foreign guest speakers. That helps to get things done.”
THE MENTOR
Every community of practice has a mentor. Jos van Kempen is a mentor of the community in Pristina. From the start in 2020, the university professor at the Institute of Business Administration and the Master Healthy Aging Professional of the Hanze University of Applied Sciences will supervise the process. Jos has just returned from Pristina, where he mentors the community towards their ideal of health. “We organized a round table in Pristina in which we talked about SUSWELL in Pristina. The mayor was invited, the media, parents of children with autism and professionals involved in care for health. In addition to developing social innovations related to health, we also develop education for specific regions and for professionals. For example, I gave a presentation to the round table on futures literacy. About the place that futures literacy can take in a social innovation and what place it could take in education in that region. Futures literacy is not about predicting the future, but about developing skills to deal with an unknown future. You can predict whether the sun will shine tomorrow, but when it comes to complex issues such as poverty, war victims, security, obesity, autism, corona… there are so many elements that come into play that you cannot predict what will come out of them. Being resilient to changes rather than trying to get a handle on that change. That is a very important skill for all those communities of practice. People are open to it. Every now and then I get a critical note. “Jos, do you think we have the luxury to think about the future and at the same time trying to survive every day.”
Growing as a teacher
Jos finds the question of what SUSWELL will bring him as a teacher a difficult one because everything has common ground. “I learn from the people in Kosovo from their hospitality and from their collectivity. They think it’s important to do things together. As a professional, I learn from the complex situation with all those stakeholders. As a teacher, I have grown in flexibility and creativity. We are used to having everything planned in education. My knowledge about futures literacy has developed enormously. I learn a lot about guiding interdisciplinary groups around complex questions, such as the issue of children with autism. For example, by simultaneously paying attention to paradoxes, such as unity and diversity. Without unity, there is no common direction, but without diversity, there is no broad view of the issue. That is sometimes quite difficult. Dealing with complexity is becoming an increasingly important skill.”
Long term
Project leader Paul Beenen emphasizes: “We want the communities of practice to work together in the long term because if you want to improve care for people with autism, for example, it might take twenty or thirty years. You don’t do that in a project. Take care of health instead of health care.” Also read Paul Beenen’s opinion article: The uncanny and destructive consequences of the breaking of dialogue in times of war.
ABOUT SUSWELL
SUSWELL consists of nine higher education institutions and six civil society organizations from seven European countries that embrace the complexities of health systems and accept the need for co-creation to enable social change. SUSWELL will run for three years, started in November 2020 and received an Erasmus+ Capacity Building in Higher Education grant. The subsidy has been stopped for the entire project because of the war in Ukraine. SUSWELL’s predecessors were the E+ funded projects COP4HL and Score. Those projects also linked health care and welfare with the same partners in the same environment.